.png)
 The recent Oceania Seating Symposium was a great opportunity for those involved in seating and mobility to come together and share the latest evidence, research and areas of knowledge. I noted that there was a large amount of attendees that were interested in the scoliotic positioning which isn’t surprising being a position we frequently see within complex postural needs so, thought it was timely to focus this month's blog on the considerations in AT to address this need.
The recent Oceania Seating Symposium was a great opportunity for those involved in seating and mobility to come together and share the latest evidence, research and areas of knowledge. I noted that there was a large amount of attendees that were interested in the scoliotic positioning which isn’t surprising being a position we frequently see within complex postural needs so, thought it was timely to focus this month's blog on the considerations in AT to address this need.
We know that lateral trunk support is required for both reducible and non reducible scoliosis presentations. Whilst the posterior support including seat to back angle and contours have a significant impact on a scoliosis and should be addressed prior to lateral support, today's session will focus on the considerations of the lateral supports.
 Lateral supports can be generalised where they essentially form an extension built in as part of the posterior shell surface. This can provide the user with a cue and can also address minimal reducible scoliosis. However once a scoliosis becomes more significant and the posterior support contours have been addressed we need to consider the laterals. With so many mounting, release, sizes and materials available how do we decide what options will best meet the users needs?
Lateral supports can be generalised where they essentially form an extension built in as part of the posterior shell surface. This can provide the user with a cue and can also address minimal reducible scoliosis. However once a scoliosis becomes more significant and the posterior support contours have been addressed we need to consider the laterals. With so many mounting, release, sizes and materials available how do we decide what options will best meet the users needs?
Mounting Laterals
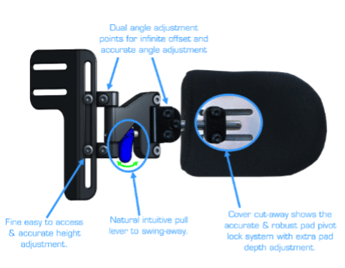
Whilst there has historically been both incremental and infinite mounting options on backrests we tend to see manufacturers addressing both options depending on the intended use of the back support. When we determine the need for individualised lateral trunk supports we need to also consider the placement options and type of Pads. Will you need to make ongoing micro adjustments to the height or do you only need a generalised position of support? Also consider how the adjustments are made. Infinite adjustment is usually achieved through a track system and often quite easy to undo and slide up or down without removing the lateral pad. Incremental adjustment requires you to take off the lateral and reset in another mounting point above or below.
Lateral Release
Laterals often have a fixed or swingaway option. Whilst a fixed option is usually more sturdy a swing away can assist in transferring tasks. Swingaway options are often springloaded, this offers a safety mechanism by preventing the lateral from unintentionally opening when a person leans on it, but requires the users weight to be off the lateral for the release mechanism to be operational. This requires either the user to independently weight shift or for additional manual handling by the person assisting them. Some manufacturers offer options to assist an individual to release the lateral independently however it is crucial that the user ensures during the trial that this can be completed as it requires upper extremity movements whilst holding weight off the lateral.
Pad Size and shape
This question comes up quite frequently during seating workshops. There are several considerations here,
- How heavily is the user loading – Is there an increased pressure risk and you need to distribute the contact over a larger surface area?
- Is it just lateral support or are you also providing some anterior support?
- How deep is the trunk - Will there be a risk of entanglement with slings?
As in all AT prescription less is often more.
Materials
Just as we must be able to critically analyse and then reason materials for backs and cushions we also need to for laterals. I have frequently received requests around adding gel to protect the user collapsing their axilla over the top of the high lateral. My first thoughts to this query are what are the contours and is the lateral placement in the right position, whilst our first thought with a scoliosis that continues is to raise the side they are leaning towards, this is often symptomatic of not quite catching the scoliosis at the lower aspects so I always tend to go back and reassess the positioning in the first instance. The materials of the support however are still crucial. When we breathe, we experience rib flare to enable expansion of the lungs. When correcting or accommodating a scoliosis we need to provide specific crucial points of control, balancing this can be tricky, the level of immersion can assist in balancing these needs.
Reducible vs non reducible scoliosis
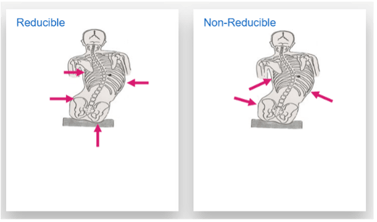 The primary difference within this presentation that we need to consider is what angle does the lateral need to interface appropriately at the trunk. When correcting an asymmetrical posture the laterals are less likely to require a rotational angle so often standard mounting will be effective. However if we are accommodating some asymmetry, rather that placing a force on the apex of the curvature we are more likely to need to rotate the laterals to prevent further asymmetry so need to be able to meet this angle. (Image from Permobil APAC Clinical Pathways workshop)
The primary difference within this presentation that we need to consider is what angle does the lateral need to interface appropriately at the trunk. When correcting an asymmetrical posture the laterals are less likely to require a rotational angle so often standard mounting will be effective. However if we are accommodating some asymmetry, rather that placing a force on the apex of the curvature we are more likely to need to rotate the laterals to prevent further asymmetry so need to be able to meet this angle. (Image from Permobil APAC Clinical Pathways workshop)
Number of laterals
We need to remember that foundational concept in seating of opposite and equal forces. A solitary lateral will not provide the required support, ideally we will need 3 laterals to achieve appropriate support though it is important to note that this third point may be from a hip guide or the length of a generalised lateral may still provide two counter points of control.
Of course whilst I have separated out these concepts they need to be considered in relation to each other not in isolation.
The simulation of the potential sitting posture within the MAT evaluation can give us crucial information to consider within the clinical reasoning process. Essentially the lateral supports will replicate the therapists hands in supporting the lateral trunk positioning but we need to consider this from the clinical needs of the user.
Author

Tracee-Lee Maginnity, BHSc (OT)
Clinical Services Specialist
Tracee-Lee Maginnity joined Permobil Australia in July 2019, as a clinical education specialist. Originally from New Zealand, she graduated Auckland University of Technology with a BHSc (Occupational Therapy) in 2003 and has since worked in various roles related to seating and mobility including assessing, prescribing and educating. After gaining experience as an assessor and prescriber at Seating To Go / Wheelchair Solutions in prescribing for both disability and injury, she moved to Australia in 2011 to take on the Senior Occupational Therapist role in a custom moulded seating service. She then worked in clinical consulting and education roles until joining Permobil. Tracee-Lee is passionate about maximising functional outcomes with end users and the importance of education within the industry. She has mentored many therapists interested in AT. Her experience includes working with complex postures to achieve custom outcomes. Tracee-Lee is also an international wheelchair rugby classifier where she enjoys the task analysis of wheelchair propulsion and functional capacity identification of athletes.