
Throughout some of my recent education sessions, I have had many conversations with therapists where the conversations and questions have started with “ … but what would you do when…?” – with the therapist often referring to having a lack of funding, social or psychological barriers, decreased client engagement or multiple carers in place – which makes prescribing the most ideal piece of Assistive Technology (AT) difficult. My response is always the same... “That is a great question, and exactly why Allied Health Professionals (OTs and PTs) prescribe complex AT.”
So how exactly do we answer this question? Well, the answer is simple, and it goes back to clinical reasoning and the core of all AT prescription – the assessment. Since my early days at University, I have generally used the Person-Environment- Occupation (PEO) model to guide my practice, however I now find that International Classification of Function (ICF) is my preferred go to.
I have often heard the team ‘within scope’, referring to whether someone’s skills align with their practice. For Australian therapists however, there are no additional credentials required to prescribe
If you want to learn more about the ICF, I encourage you to have a look at the WHO website here.
Working in the real world, means that you as the prescribing therapist are keeping the client at the centre of your clinical reasoning. If prescribing the gold standard or “textbook” piece of AT is not doable for whatever reason due to a barrier in place, an in-depth assessment will assist you with your clinical reasoning process and ultimately you will prescribe the best piece of AT for the individual (and that is why there are so many choices on the market - because one size does not fit all).
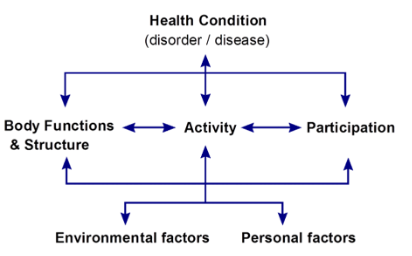
Using a model such as the ICF or PEO will assist you with your clinical reasoning process and assessment as it ensures that you gather all the information that you need and helps you to categorise the information into Person, Environment and Occupation and establish and prioritise the individual goals.
We might sometimes think that prescribing a pressure care cushion is reasonably simple – and a piece of AT which should be easy to use. However, I know that I am not the only therapist who has gone out to a review and the client is sitting on a cushion which is upside down and back to front. Clinical reasoning assists us with the real-world prescription. For example - if we are wanting to prescribe a pressure care cushion for a client who we have determined is at high risk of developing a pressure injury, using a model such as the ICF will assist us with the reasoning and prescription.
Through the assessment process, you may know that the person you are working with is at high pressure risk, however they may also have reduced problem-solving skills, multiple carers (perhaps from a casual pool), inconsistent positioning and you have observed that simple equipment has been implemented well previously. Functionally, the client transfers well with 1 x assist and your hypothesis from your assessment is that you want a cushion which has both a high level of immersion under the ITs and sacrum – but needs to be flat or slightly contoured at the front of the cushion to maximise stability and maintain the individuals transfer status.
Your concerns when considering prescribing the gold standard hybrid style cushion which has air, fluid or gel in the well of the cushion and high density foam at the front of the cushion, is that due to the inconsistent positioning of the client and the high number of casual staff, that the cushion will not be maintained as required or checked to make sure the client is sitting in the cushion, and not on the hard high density foam at the ischial shelf. A full air or gel cushion would be a great next option; however, the client is unable to check for bottoming out and/or appropriate inflation, and the carers are not confident either. Working in the real world sometimes means prescribing what is going to work daily and something that will be used as intended. Although as the prescribing therapists we would ideally like to prescribe a hybrid style cushion or a full air cushion, we may in a case like this end of prescribing a great foam-based cushion. Although, it may not provide as much immersion as an air or gel cushion, by prescribing a foam cushion we are removing the need for maintenance and perfect positioning every time. Would I classify this as the textbook or gold standard of cushions? From a textbook perspective this would probably not be considered “gold standard” – for this individual in this example, it actually is, as it was the clinical reasoning process and assessment which got us to this specific prescription. This cushion is going to meet the goals and minimise the pressure risk as it will be used consistently and as prescribed. – Yes, I am going to write front, back, bottom and top of the cushion and every cover on the cushion too!
We work with people in our roles. Every person is as individual as you and I are. Which means each person’s goals are different and what we recommend will be different. Be clear on what your goals and clinical reasoning are. Work with the individual, their environment and their occupations. This will ensure that you are prescribing the most appropriate piece of AT that you can. Whether you are prescribing a cushion, backrest or a Power Wheelchair – remaining client focused, completing an in-depth assessment and setting clear goals (and prioritising them) will ensure you are prescribing the best piece of AT that will work for that individual.
Author

Tilly Brook, MOccThy (Hons) (OT)
Clinical Services Specialist
Tilly Brook graduated from the University of Adelaide in 2008 with a Bachelor of Health Science followed by a Masters of Occupational Therapy (Hons) in 2010 from the University of Sydney. Tilly worked within rehabilitation, working primarily with adults with a brain injury until 2015 when she moved to Singapore. In Singapore, she worked with children and adults at the Cerebral Palsy Alliance School (CPAS). In 2017 Tilly’s clinical knowledge continued as she worked with Mobility Solutions in Auckland, New Zealand. On her return to Australia, Tilly assisted in the development of the Clinical Hub Team at Sunrise Medical where her passion and experience for mentoring and educating therapists grew. Tilly Joined Permobil in January 2022 and is driven to grow therapists, enabling them to be the best therapist they can be.